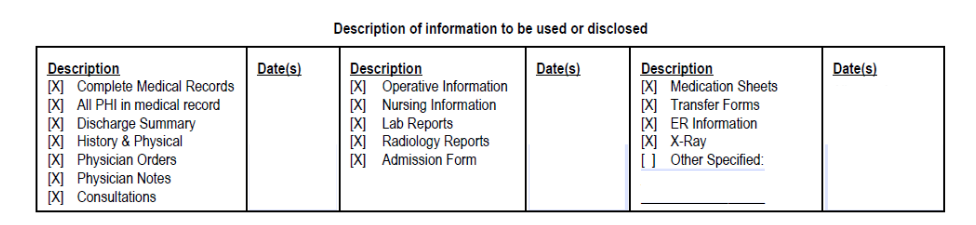
Please release to A Act of Love/Alternative Options and Services for Children (“Act of Love”), or any employee or agent of Act of Love, 9561 South 700 East, Suite 101, Sandy, Utah, 84070, copies of all my medical records, including, but not limited to charts, notes, evaluations, test results, invoices and similar documents that you have in your possession as are described below. These records are needed by Act of Love in connection with an adoption of my child. I hereby release and absolve you from any and all liability for providing such information to Act of Love.
I understand that this information may include, when applicable, information relating to sexually transmitted disease, Human Immunodeficiency Virus (HIV infection, Acquired Immune Deficiency Syndrome or AIDS Related Complex) and any other communicable disease. It may also include information about behavioral or mental health services, and referral or treatment for substance use disorder (as permitted by 42 CFR Part 2).
This disclosure and use is for the following purpose: Adoption matter.
This information may be disclosed to and used by the following categories of persons or organizations.
Attorney(s) for adoptive parent(s) Adoptive parent(s)
Agency for adoptive parent(s) Court in connection with adoption, as necessary
Interstate Compact on the Placement of Children, as necessary
I understand that I have a right to revoke this authorization at any time. I understand that if I revoke this authorization I must do so in writing and present my written revocation to youment. I understand that the revocation will not apply to my insurance company when the law provides my insurer with the right to contest a claim under my policy. Unless otherwise revoked, this authorization will expire one year from the signature date.
I understand that authorizing the disclosure of this health information is voluntary. I also understand that I may refuse to sign this authorization and that my refusal to sign will not affect my ability to obtain treatment, payment for services, or eligibility for benefits.
By signing this Authorization, I understand that any disclosure of information carries with it the potential for an unauthorized redisclosure and the information may not be protected by federal privacy rules. I further understand I have the right to receive a copy of this signed authorization. I understand and agree that a photo-copy
